Квадратная мышца поясницы упражнения
Содержание:
- Quadratus Lumborum Tightness: Postural Mistakes
- INDICATIONS
- Techniques[edit | edit source]
- Диагноз
- Quadratus lumborum Stretch
- Author’s Pick
- What Causes the QL to Tighten Up?
- A healthy relationship on the mat
- Simple problems with simple answers
- Quadratus Lumborum Kası Nedir?
- 3 Quadratus Lumborum Stretches
- A Tight QL and Serious Back Problems
- A knock-on effect
- Function[edit | edit source]
- References[edit | edit source]
- PATIENT POSITIONING AND EQUIPMENT SELECTION
- How To Release QL Tightness
- Quadratus Lumborum’un İşlevi
- Quadratus Lumborum Functions
Quadratus Lumborum Tightness: Postural Mistakes
My goal is for you to not only release the QL but to avoid developing this tightness in the first place. Below are the most common causes of quadratus lumborum tightness.
Another great resource to learn how to fix back pain permanently is the Back Pain Control program.
Prolonged Sitting
The first common cause of quadratus lumborum tightness is prolonged sitting without adequate lumbar support. We’re usually busy and don’t pay too much attention to our posture.
Being mindful of this will pay off in the long run.

The back muscles will bear the load if you sit for hours every day. Maintaining good posture and placing a lumbar support behind your back will help you avoid this tightness.
Resource: How to sit without irritating your hips and lower back.
Leaning To One Side
A second common cause is sitting and leaning to one side.

And we usually tend to have a preferred side to lean on.

It’s very common to sit in the passenger seat and start leaning on the hand rest.
During our last road trip, we drove for more than 15 hours. At one point, I had to make a huge effort to maintain a good posture and avoid side leaning.
Related: 15 tips to drive without lower back pain
Doing this automatically puts more tension on the QL muscle on that side.
While doing it on purpose to accomplish a goal (picking something up, exercise, quickly reaching for an item) not have a negative effect, maintaining this posture for a long time and doing it repetitively would certainly tighten up the QL in the long run.
And, sure enough, when we got to our end destination, I definitely felt more tightness in my lower back area.
I spend a few minutes releasing it and doing core exercises and it got better. I have the QL release tutorial I did below.
Sleeping Posture (with one hip hiked up)
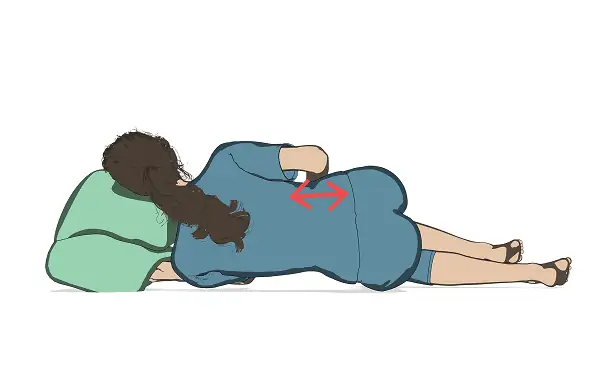
Hiked up hip tightens up the QL muscle.
Your posture at night is just as important as your posture during the day. We spend hours sleeping.
And that has an effect on our muscles and joints.
A sleeping posture that can certainly contribute to QL tightness is sleeping with your hip hiked up.
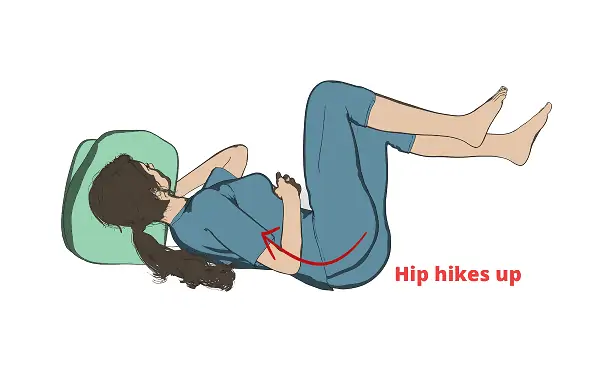
The right QL will be more prone to tightness.
It’s so easy to get into that comfortable position and curl up into a ball. But, be careful to always stabilize your pelvis and make sure your hips are aligned.
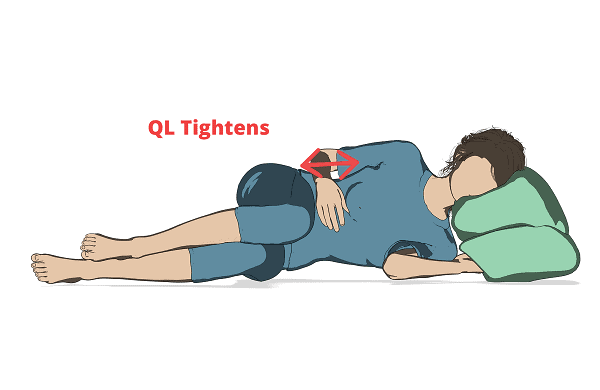
In addition, notice how your body gets into that C position when you sleep on the side and rest your head on high pillows.
Overtime, holding this posture for hours every night can shorten the QL and create chronic tightness.
I have a step-by-step post on the best sleeping postures to avoid hip, lower back, and neck pain.
Side Bending To Compensate During Exercise
Chronic tightness can also be caused by side bending from compensation during certain exercises. You may not notice this at first.
For example, when performing the side-to-side glute activation walks, many people start to bend to drive the movement (I’ve seen this many times at the gym).
(I demonstrate this compensation pattern in the video tutorial below)
This side bending engages the QL muscle and leads to tightness, or it can at least contribute to it.
There are many reasons why people compensate during this exercise:
- The band is too tight and they have to use their back to push through the movement.
- Weak glutes that can’t execute the movement with resistance (using a lighter band usually helps).
- Simply not knowing how to do this exercise with proper form. I’ve seen a lot of personal trainers not correct their clients when they engage in this flawed movement.
Compensation can usually be fixed simply by learning how to do the exercise with proper form, and understanding what you’re trying to achieve by doing the exercise.
For example, to avoid engaging the QL in the example above, learn that the glute medius abducts the hip. No side bending should happen to “help out”.
You want to keep your back stable and straight, and only move your legs side to side. Moving your upper body to help will only reduce the effectiveness of the exercise.
INDICATIONS
Most of the indications for QL nerve blocks are based on case reports and clinical anecdotal experience. There are no studies comparing the safety and efficacy of the three types of QL nerve block. Table 1 compares and summarizes the three types of QL nerve blocks.
TABLE 1.Main features of QL nerve blocks.
| QLB1 | QLB2 | TQLB | |
|---|---|---|---|
| Clinical indications | Abdominal surgery below the umbilicus. | Abdominal surgery either above or below the umbilicus (any type of operation that requires intra-abdominal visceral pain coverage and abdominal wall incisions as high as T6) | Abdominal surgery either above or below the umbilicus (any type of operation that requires intra-abdominal visceral pain coverage and abdominal wall incisions as high as T6) |
| Dermatomes covered | L1 | T4 to T12-L1; blocks the anterior and the lateral cutaneous branches of the nerves | T4 to T12-L1; blocks the anterior and the lateral cutaneous branches of the nerves |
| Lower extremity weakness | Not reported | Not reported | Potential |
| Spread to lumbar plexus | Not reported | Not reported | Potential |
| Needle entry and approach | Lateral abdomen near the posterior axillary line, below the costal margin and above the iliac crest and inserting the needle inplane with the curved array probe oriented axially. | Lateral abdomen near the posterior axillary line, below the costal margin and above the iliac crest and inserting the needle inplane with the curved array probe oriented axially. | Lateral abdomen near the posterior axillary line, below the costal margin and above the iliac crest and inserting the needle inplane with the curved array probe oriented axially. |
| Potential complications | Complications are related to the lack of anatomical understanding and needle expertise. It is possible to puncture intra-abdominal structures such as the kidney, liver, and spleen. | Complications are related to the lack of anatomical understanding and needle expertise. It is possible to puncture intra-abdominal structures such as the kidney, liver, and spleen. | Complications are related to the lack of anatomical understanding and needle expertise. It is possible to puncture intra-abdominal structures such as the kidney, liver, and spleen. |
| Injection site | Potential space medial to the abdominal wall muscles and lateral to QL muscle, anterolateral border of the QL muscle, at the junction with the transversalis fascia, outside the anterior layer of the TLF and fascia transversalis | Posterior to the QL muscle, outside the middle layer of the TLF | Anterior to the QL muscle, between the QL and the psoas major muscles, outside the anterior layer of the TLF and fascia transversalis, close to the intervertebral foramen |
| Level of difficulty | Intermediate | Intermediate | Advanced |
The various QL nerve blocks share the same indications as of the TAP nerve block. Some examples are as follows:
- Large-bowel resection, open/laparoscopic appendectomy, and cholecystectomy
- Cesarean section, total abdominal hysterectomy
- Open prostatectomy, renal transplant surgery, nephrectomy, abdominoplasty, iliac crest bone graft
- Ileostomy
- Exploratory laparotomy, bilateral nerve blocks for midline incisions
NYSORA Tips
• Close to the transverse process, the QL muscle appears thin as it is visualized anterior-posterior; visualized from the flank, the muscle looks much broader.
• Use color Doppler before insertion of the needle to detect the lumbar arteries on the posterior aspect of the QL muscle or any other large vessels.
• The QL is identified medial to the transversus abdominis muscle. The latissimus dorsi and erector spinae muscles are superficial and more hyperechoic.
Techniques[edit | edit source]
Related Pathologiesedit | edit source
Dysfunction of the lumbar structures whether degenerative, neuropathy, and/or inflammatory, may contribute to poor muscle firing and weak stabilization by the QL.
Lumbar spine pathologies like bulging discs, and facet joint hypertrophy from chronic inflammation may effect nerve conduction and response to the QL and Iliopsoas resulting in poor muscle stabilisation and mechanical stress from chronic contracture.
Moaratty-Koehler Syndrome (MKS) is another condition related to QL dysfunction.
Treatmentedit | edit source
|
https://youtube.com/watch?v=OxJzVs738Oo%3F |
https://youtube.com/watch?v=Xjg6Gkla03g%3F |
|
https://youtube.com/watch?v=m-U4X9R4JDo%3F |
https://youtube.com/watch?v=22B2SpMpoUQ%3F |
Диагноз
Клинический диагноз миофасциальной боли в принципе зависит от врача, который может предположить эту причину, как возможную, для объяснения природы боли. Миофасциальные болевые синдромы боли могут быть похожими на большое количество других заболеваний, поэтому необходимо провести адекватное обследование. Миофасциальная боль характеризуется, как не интенсивное глубокое ощущение боли, которое усиливается при работе заинтересованных мышц и стрессах, что увеличивают ригидность мышц. Характерная клиническая особенность миофасциальной боли — обнаружение триггерной точки. Это — четкий очаг локальной болезненности в пределах мышцы. Иногда боль при пальпации может распространяться и воспроизводить симптомы у пациента. Но как правило, иррадиация боли не идет по тем же путям, что и кожная иннервация корешком. Пальпация обычно выявляет веревкообразное уплотнение мышечных волокон, часто называемых “тугой связкой”. Иногда, быстрый щелчок по этой связке или прокалывание иглой триггерной точки приводят к судорожному сокращению заинтересованной мышцы. Эта конвульсивная реакция может быть выявлена только в поверхностных мышцах. Миофасциальная боль часто следует за травмой мышцы или повторяющимися нагрузками. Нередко в современных клиниках проводились многочисленные дорогостоящие обследования, прежде чем выставлялся диагноз миофасциальной боли. У некоторых пациентов с наличием четкой причины скелетно-мышечной боли (например, ревматоидный артрит), может развиться миофасциальный болевой синдром который не диагностируется так, как есть основное заболевание. У миофасциальной боли есть определенные клинические особенности, которые помогают в постановке этого диагноза. Боль, как правило, описывается, как глубокое болевое ощущение, часто с чувством скованности в вовлеченной области; иногда это рассматривается как скованность в суставах. Миофасциальная боль усиливается при нагрузке заинтересованной мышцы, стрессов, воздействия холода или постурального дисбаланса. Иррадиация от триггерной точки может быть описана, как парестезия, таким образом быть похожей на симптомы при радикулопатии (поясничной или цервикальной). Слабость мышцы, возникающее вследствие ее малой нагрузки может привести к таким симптомам, как быстрая утомляемость, нарушение координации движений, нарушения сна. Пациенты с миофасциальной болью, вовлекающей мышцы шеи и лица, могут испытывать симптомы головокружения, шума в ушах и нарушения статики.
Характерные особенности миофасциальной триггерной точки:
- Фокус болезненности при пальпации заинтересованной мышцы
- Воспроизведение жалобы на боль при пальпацией триггерной точки (с усилием около 3-кг)
- Пальпация выявляет индурацию (уплотнение) смежной мышцы
- Ограниченный диапазон движения в заинтересованной мышце
- Часто псевдослабость заинтересованной мышцы (без атрофии)
- Часто отраженная боль при длительном (~5 секунд) давление на триггерную точку.
Quadratus lumborum Stretch
Self Quadratus Lumborum stretch : Sitting side bends
- 1. Sit comfortably, with your spine lengthened. Place a towel or stretching strap under your right foot, and hold the other end in your right hand. Side band to the right side as far as you can, taking up any slack in the stretching strap. This lengthens the left Quadratus lumborum.
- 2. Using the stretching strap to prevent your motion, try to sit up straight, isometrically contracting left quadratus lumborum for 6 seconds as you keep breathing normally.
- 3. After the isometric contraction, relax, breathe, and deepen the stretch by bending farther to the right.
Quadratus Lumborum stretch in Supine position
- 1. The patient is supine on the table. The physiotherapist firmly grasps the right foot and ankle and passively stretches the entire leg to pull the hip down, then across the midline, lengthening the QL on the right.
- 2. From this starting position, the patient attempts to hip hike ( pull the hipbone towards the head). Be sure he is not lifting the leg toward the ceiling (hip flexion). Hold this isometric contraction of the QL for 6 seconds as the patient breathes normally.
- 3. After the isometric push, the stretcher relaxes and inhales deeply. As he relaxes, maintain the leg in the starting position.
- 4. As he relaxes, passively stretch the leg down and across the midline farther, deepening the right quadratus lumborum stretch.
- 5. Repeat 4-5 times.
Quadratus Lumborum stretch in side lying position
Read research articles relating Quadratus lumborum and low back pain on PubMed
- 1. The patient is lying on his left side, with his back at the edge of the table and his right leg hyperextended and hanging over the edge of the table. He has his left leg bent and as close to his chest as possible. Be sure he keeps his hips stacked vertically on top of each other. He reaches his right arm up over his head. This lengthens the right QL. If the patient experiences any low back pain in this position, he may bend forward from the waist to round his low back while keeping his leg hanging off the edge of the table.
- 2. Physiotherapist stands behind the patient. He crosses his arms and places his left hand against patient’s right iliac crest; right hand is spread wide and placed on the lateral aspect of rib cage. This cross hands position gives a better mechanical advantage to resist the isometric contraction of QL.
- 3. Patient education begins now. Patient contracts the right QL by bringing the hip and the ribs towards each other. He is side-bending and hiking his hip at the same time.
- 4. Once the patient can perform the motion, ask him to begin slowly to try to bring the top of his hip and rib cage toward each other. Physiotherapist applies matching resistance to prevent any motion from occuring. Control the force of his effort.
- 5. After the isometric push, the patient relaxes and inhales deeply. As he relaxes, allow his leg (and his leg) to drop towards the floor.
- 6. As he exhales, ask the patient to pull his foot closer to the floor and reach farther up over his head to increase the stretch on the right QL.
- 7. Repeat 4-5 times.
|
Author’s Pick
Rating: 4.4 Votes: 252 |
What Causes the QL to Tighten Up?
You can’t win when you’re dealing with a tight QL; inactivity and overuse can both cause a tight QL. The key issue is chronic forward flexion: whether you’re sitting still or riding a bike, maintaining forward flexion for long periods can create tight QL muscles [].
The back surgery I had when I was in high school left me with a contracted right side – the side where the scar is. Because of this, my right shoulder is lower than my left and before doing any exercise; I always lengthen the right QL to achieve symmetry, especially with any axial loading exercises like Squats or Deadlifts.
This is just something I have to do before training and it won’t go away because it’s related to the huge scar I have from going under the knife that will never be as elastic as normal skin.
A healthy relationship on the mat
The most effective way to support a healthy relationship between all four of these muscles is with the Constructive Rest Posture.

Constructive rest pose
- Internal rotation of the femurs gently stretches the tight piriformis muscles.
- Knees lifted in a bent and supported position allows the sacrum, with the aid of gravity, to nestle its way into its rightful place between the two ilium bones. The relaxation of the iliac here is rooted by the resettling of the two iliums.
- The slight posterior tilt of the sacrum- ilium/pelvis allows for the gentle stretch of both quadratus lumborum and iliopsoas.
Resting in this posture for a lengthened period of time is key in order to allow gravity to be a help in softening and relaxing without unnecessary holding and tension. Happy and healthy these four muscles will be!
Simple problems with simple answers
Muscles that are tight (locked SHORT) from repetitive forward flexion: the psoas and iliacus.
Iliacus(major hip flexor)
- Originates: Iliac Fossa (internal rim and surface of ilium)
- Inserts: Lesser Trochanter of Femur (medial superior femur)
Muscles that are tight (locked LONG) from repetitive forward flexion: the QLs
Quadratus Lumborum (deep spine extensor to neutral when both are working)
- Originates: Posterior Internal Iliac Crest
- Inserts: Lumbar Spine 1-4 and Lowest Rib
Quadratus Lumborum
Like a relationship between two people that may need a bit of counselling to regain balance, the simplest dilemma in this region of the body is that the iliacus and psoas (known together due to their combined insertion on the femur as iliopsoas) are tight and weak from overflexing and the quadratus lumborum are tight and weak from trying so hard to bring the body back upright to neutral.
The answer here is as equally simple: stretch and strengthen these pairs (agonists and antagonists) with backbends and quadricep stretches.
Unfortunately for most of us the dilemma is much more complicated than this.
Quadratus Lumborum Kası Nedir?
Quadratus lumborum , karnın derinliklerinde yatan ve bel omurgasının her iki yanında yer alan dikdörtgen şeklinde bir kastır. QL, daha büyük kasların altında ve böbreklerin üzerinde yer alan derin bir bel kasıdır.
Fonksiyonel olarak QL, omurganın ve pelvisin stabilizasyonuna katkıda bulunur. Bir taraftaki kası bükmek gövdeyi bu yöne doğru bükerken her iki tarafın da bükülmesi omurgayı uzatır. QL ayrıca göğüs kafesi hareketleri sırasında on ikinci kaburgaya sabitlenir ve nefes verdiğinizde yardımcı bir kas görevi görür.
Quadratus lumborum, lomber omurgayı (alt sırt=bel) stabilize etmek için iliopsoas, lomber paraspinaller ve çeşitli ligamentlerle çalışan bir ekip olarak işlev görür.

(Paraspinal kaslar, erector spinae denilen sırtınızı destekleyen üç kas grubundan oluşur. Bu üç kas alt omurgadan boyuna kadar uzanarak işlev görürler.)
3 Quadratus Lumborum Stretches
QL Wall Stretch

- You want to stand with your side against the wall. Your hip touching the wall.
- Raise your arm up that’s against the wall. Lead to the side and move forward and at an angle.
- You should feel a nice stretch on the QL as well as the latissimus dorsi muscle.
Child Pose Stretch

- Get down into the child pose position.
- From there, reach out with your arms and move your arms to one side. hold the stretch for 10-20 seconds, then slowly move your arms to the center, and then to the other side.

This nice QL stretch will also release lower back tension and help decompress the lumbar spine.
90 Degree Stretch
This is a great glute stretch. And with a small twist, we can target the QL muscle as well and release it.

- Get into the 90-degree stretch position.
- Make sure your front and back leg are at a 90-degree angle.
- Lift your arm up (the front leg side).
- Bend your body to the side to elongate the side of your back.
- Reach out diagonally. You should feel the side of your back stretching (where the QL muscle is located).
- Switch sides…

A Tight QL and Serious Back Problems
The constant sideward stress of a tight quadratus lumborum creates a shearing motion in your lumbar and sacral vertebrae that can result in crippling back injuries.
Depending on the degree of tightness and the length of time you go without correcting the issue, you can suffer from:
Compression of the S1 nerve (a pinched nerve) which besides causing intense pain all the way down to your calf, can weaken your whole leg and make it hard to even lift your heel off the ground
Degenerative disc disease, which is usually the natural breakdown of your discs with age, except tight QL muscles are making it happen much faster. Once you’ve suffered from degenerative disc disease the damage can be permanent
Scoliosis, a deformity that occurs when the spine is abnormally rotated and curved sideways. The constant pull from your tight QL will put a persistent curve in your spine that will cause major health problems

A knock-on effect
When the piriformis is tight
It pulls on the sacrum (SI Joint issues may arise), can pinch the sciatic nerve, and can cause iliotibial band tightness, due to the increase workload of the tensor fascia lata to bring the femur back to neutral with internal rotation.
When the iliacus is tight
Consistently over time, it pulls the ilium (hip bones) forward and away from the sacrum, which leads to either SI joint pain and instability and/or opposite side piriformis tightness. This then leads to IT Band tightness due to tensor fascia lata trying to bring the femur back to neutral with internal rotation.
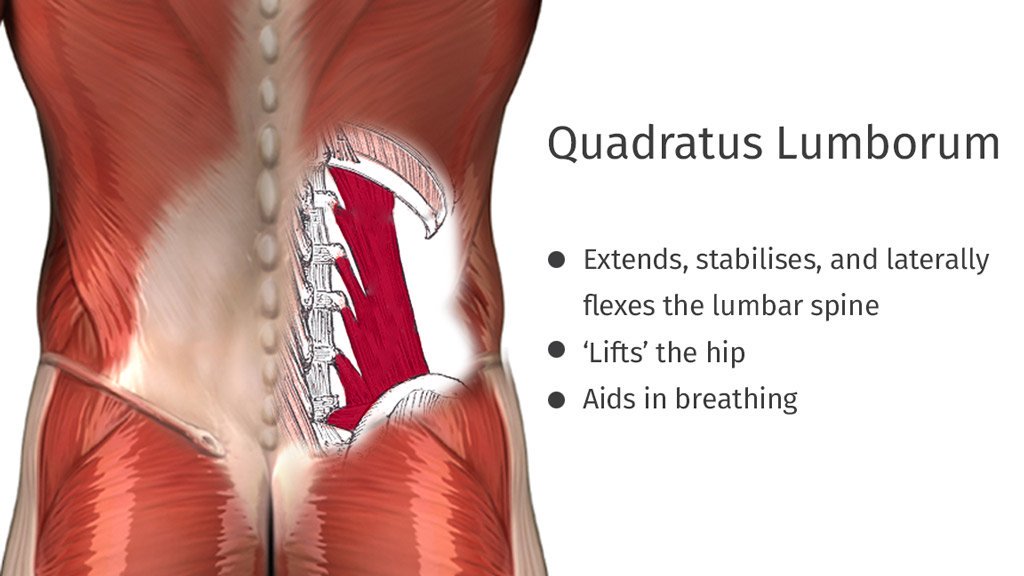
Function[edit | edit source]
Actionsedit | edit source
- Quadratus Lumborum fixes the 12th rib to stabilize diaphragm attachments during inspiration
- Lateral flexes the vertebral column
- Extends lumbar vertebrae
- It forms with the contralateral Tensor fascia lata and Gluteus medius a lateral myofascial sling which aims to maintain frontal plane stability of the pelvis.
Functional Contributionsedit | edit source
- The primary antagonist to each quadratus lumborum muscle is the quadratus lumborum muscle on the other side of the body
- The muscle group is considered a postural muscle group
- It’s one of the muscles that tends to be tight and overactive
References[edit | edit source]
References will automatically be added here, see adding references tutorial.
- ↑
- ↑ Keith L. , Anne M. R . Clinically Oriented Anatomy 7th edition. philidephia : Lippincott Williams & Wilkins.2017
- ↑
- Morgan J. Modern Principles of Core Training. Lulu.com, 2010
- McCall P. Cutting Edge: Training the Fascial Network (Part 2). Sign.;888:825-3636.
- Wallden, M. (2014). The middle crossed syndrome – New insights into core function. Journal of Bodywork and Movement Therapies, 18(4), 616–620. doi:10.1016/j.jbmt.2014.09.002
- Page .P, Frank C, Lardner R. Assessment and Treatment of Muscle Imbalance: The Janda Approach .Champaign . Human Kinetics. 2010.
- ↑
PATIENT POSITIONING AND EQUIPMENT SELECTION
For QL nerve blocks, the lateral decubitus position is preferred over the supine position as it provides better ergonomics and relevant sono-images of the neuraxial structures. A low-frequency (5- to 2-MHz) curved array ultrasound transducer in transverse axis is preferred to visualize the three lateral abdominal wall muscle layers and the QL muscle.
A 22-gauge, short-bevel needle is recommended for the single-injection technique, whereas an 18- to 21-gauge, 10-cm Tuohy needle with extension tubing is used for catheters. A peripheral nerve stimulator may be useful as a warning sign to prevent further needle advancement should the needle be mistakenly placed too deep and next to the lumbar plexus.
Learn more about Equipment for Peripheral Nerve Blocks
How To Release QL Tightness
Grab a massage ball (A tennis ball works too!).
Find the quadratus lumborum muscle. (I already covered how to find and release the QL muscle here. Below is a quick summary)
You can do this by standing straight, placing your hands around the back of your hips…

Then from here, bend laterally to the right or left side. You should feel the QL engaging to laterally flex the spine.
Place the ball on the muscle and lean against the wall.

Disclaimer: Avoid placing the ball on your spine or rolling on your spine. Never do this. We want to always stay on the muscle. Stop the exercise if you get nerve pain, numbness, or any shooting pain. If you stay on the QL muscle, you should be fine.

I start from the thoracic spine area (lateral to the spine) and slowly move down. That area tends to be very tight in general.
When you roll on an area that feels very tight, stop and take a few deep breaths while slowly rolling up and down to release that tightness.
It should feel like you’re pushing the tightness down and after a while, you’ll feel a great relief. Make sure to not foam roll your lower back area.
Quadratus Lumborum’un İşlevi
Quadratus lumborum’unuz birkaç şekilde çalışır:
- Alt omurgayı yana doğru büküyor. (lower spine lateral fleksion)
- Gövdeyi döndürür.
- Pelvisinizi stabilize eder yani sabitler.
Örneğin, bir elinizle ağır bir çanta taşırken karşıt taraftaki QL’niz sizi düz tutmak için zorlu bir şekilde kuvvet üretir. Patlayıcı fırlatma veya tekmeleme işi yaptığınız, QL’nuz gövde konumunu korumak için sert bir şekilde esner ve vücudun her yerine güç aktarmak için omurganın dengelenmesini sağlar. (yani core kası olarak stabilizasyon sağlar.)
Kritik olarak, QL yürüdüğümüzde karşı taraftaki gluteal (kalça) kaslarıyla çalışır, bu yüzden bu kaslar zayıf olduğunda diz üzerine aşırı baskı uygulayabilir çünkü hareket şekli dengesizleşir ve merkez kasların, kalçaların stabilitesini kaybetmesine neden olur.

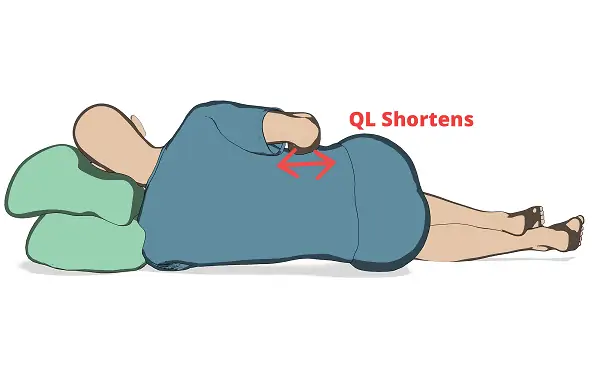
Sıkı Quadratus Lumborum ve Kalça İlişkisi
Sıkı olan QL tarafında lateral rotasyon olarak da bilinen uzunca etkilenen bir kalça; Bir kalça diğerinden daha yükseldiğinde, yükseltilmiş taraftaki bacağı fonksiyonel olarak kısaltır. Bu, pelvisin tepesini ve kalçayı göğüs kafesine doğru çeken sıkı bir QL’un sıkca belirtisidir.
Kısaca QL gerginliği belin o tarafını kısaltır, bel bölgesinde strese neden olur ve potansiyel olarak şiddetli sırt ağrısına ve skapular problemlere devamında düşmüş omuzlara neden olur. Bu bölgede ki sürekli çekme diz, ayak bileği ve bel ağrılarına neden olacaktır.
Quadratus Lumborum Functions
The Quadratus Lumborum is known for its contribution to stabilize and control the movements of other structures like the pelvis and the spine. There are few more functions that it performs which are:
- A two-sided tightening of the Quadratus Lumborum leads to expansion of the lumbar vertebral column. When the muscle gets stimulated on one side, the trunk is bent towards that direction which is called the lateral flexion.
- In addition, it helps in fixing the 12th rib when the thoracic cage movements are in action.
- The Quadratus Lumborum assists the diaphragm in inhalation.
- It helps in elevation of the Ilium bone through the ipsilateral contraction.